Techniques for Abdominoplasty and Surgical Management

Full Abdominoplasty with Muscle Repair and Liposuction
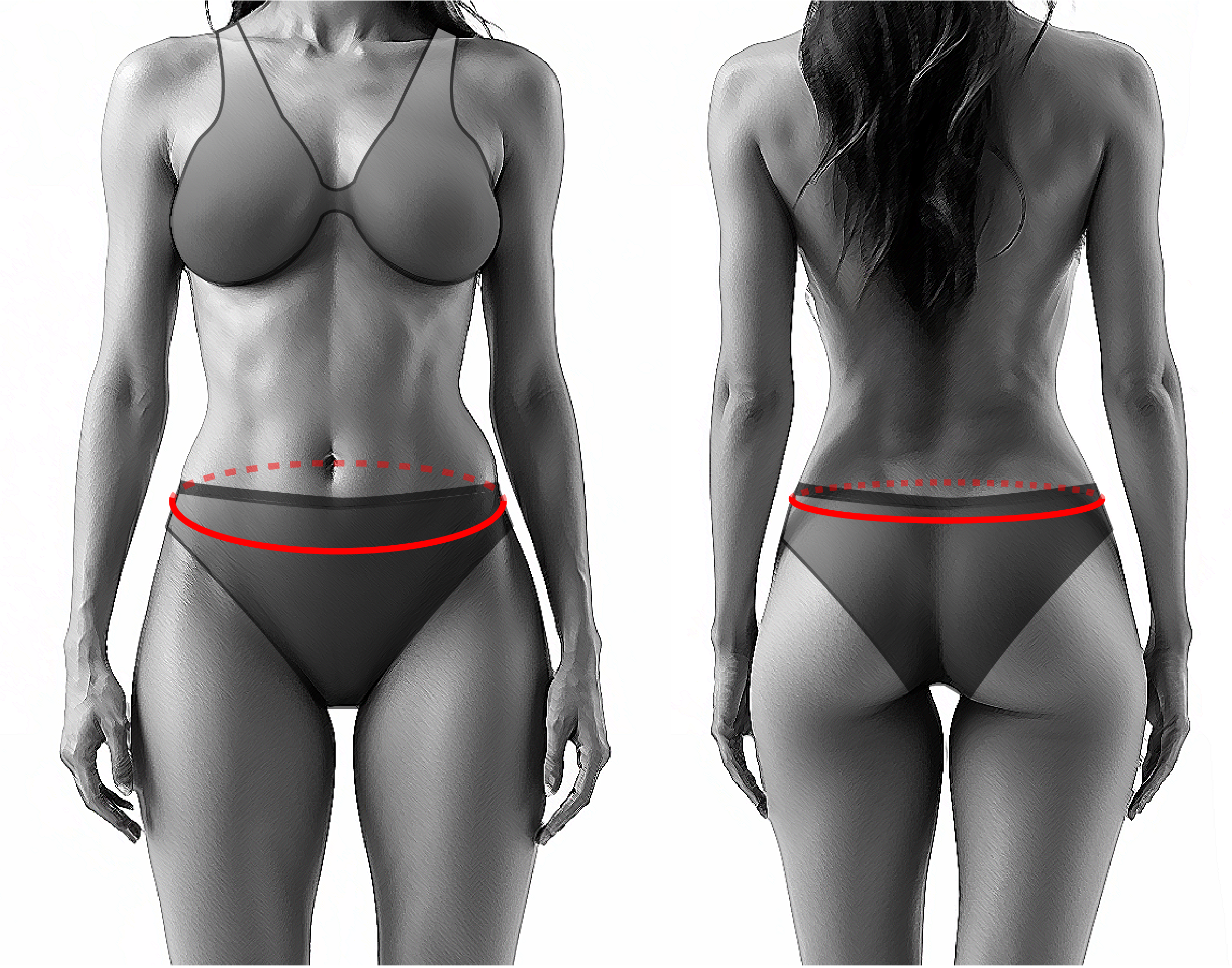
Full abdominoplasty or tummy tuck is the most performed type of abdominoplasty. The classic patient presents with skin redundancy below and above the umbilicus. The resection pattern is carried above the umbilicus and a new umbilical opening is created. The scar is placed low at the anterior abdomen, 5-7 cm above the top of the labia. These patients also present with moderate to severe muscle separation and require surgical reattachment of the recti muscles. Fatty tissue is treated with liposuction of the anterior and lateral abdomen. Modern abdominoplasty dictates lipo contouring by achieving troughs and valleys. It is also important to defat and lift the mons pubis. In some cases where the umbilicus is high to begin with or the skin redundancy below the umbilicus is not that severe, there will be a short vertical scar to offset the tension at the closure. The umbilicoplasty is preferentially performed with the 4 flap technique. This way depth is achieved and there is no external scar. The umbilical opening is performed through a cruciate incision.

Mini Abdominoplasty with Muscle Repair, with or without Umbilical Float and Liposuction
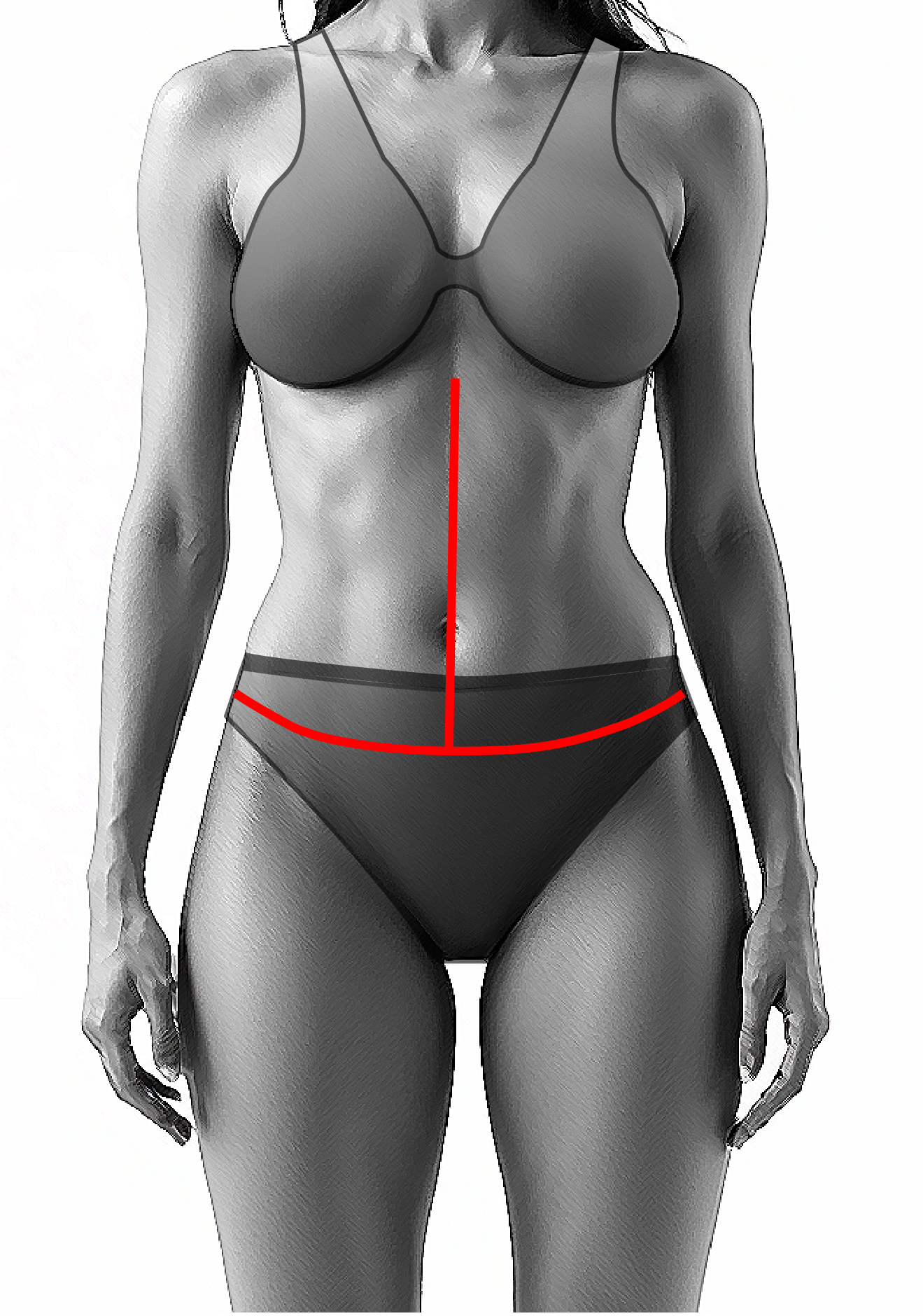
Patients that benefit from a mini abdominoplasty or mini tummy tuck have minimal skin redundancy in the lower abdomen. In this case a wedge of skin and fat is removed. There is no new umbilical opening created. The umbilicus is left as is or is “floated” to a slightly lower position. Plication of the muscles is based on individual needs. In some cases plication of the muscles is performed only below the umbilicus. In other patients, the umbilical stalk is amputated at its base to perform plication of the muscles above the umbilicus too and it is re sutured at the abdominal wall. Liposuction is performed as needed.
Lower Body Lift or Circumferential Abdominoplasty
Patients that present with excess skin and fat not only anteriorly but extending laterally and posteriorly to the back, are better served with a circumferential abdominoplasty or lower body lift. The anterior component is the same as the full abdominoplasty. The scar extends to the side and back, as a continuation of the anterior scar. This way rejuvenation of the hips and buttocks is achieved. Liposuction of the entire back is performed and in some cases fat transfer to the buttocks is performed.
Fleur-de-Lis Abdominoplasty
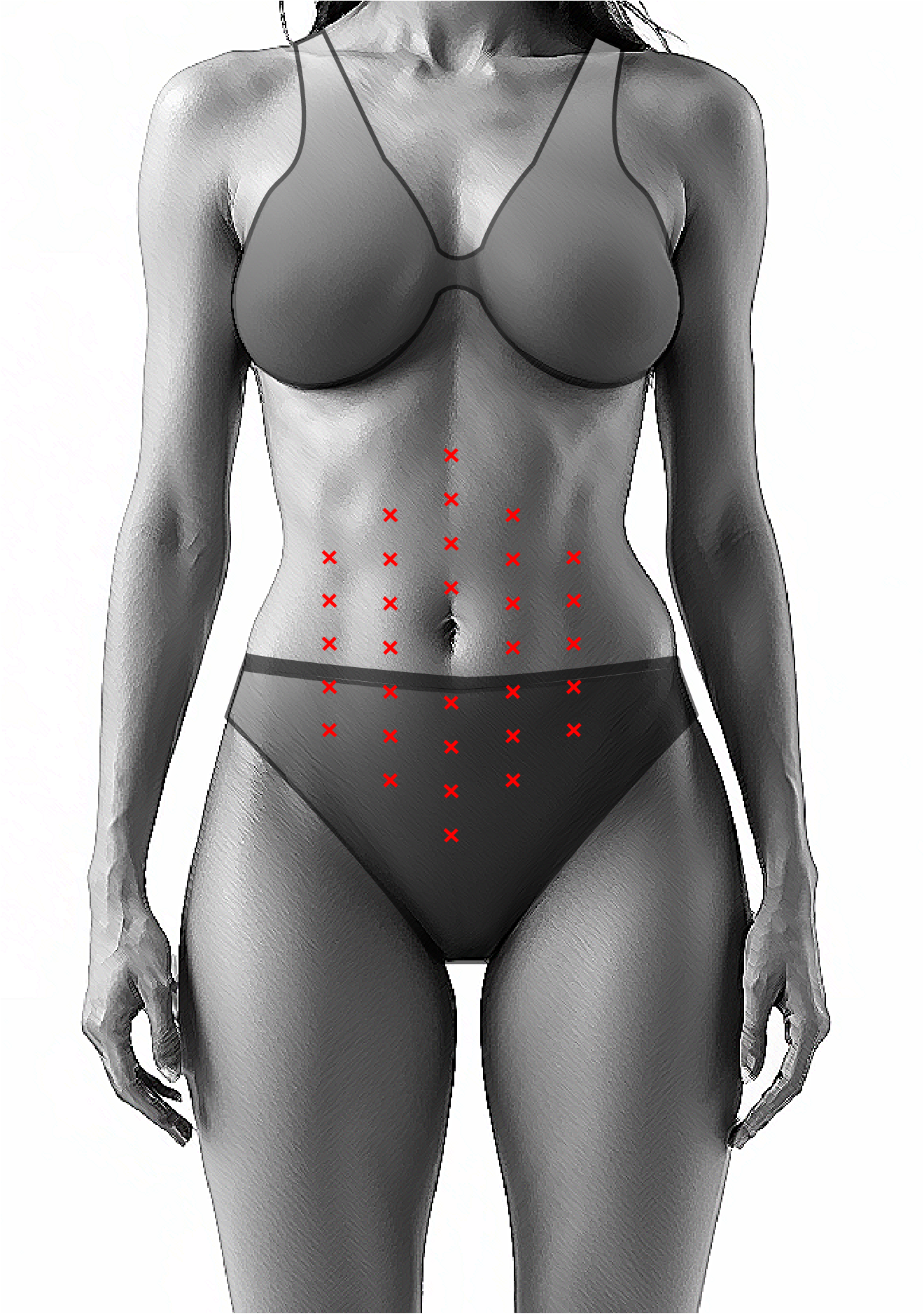
Patients with massive weight loss benefit from a Fleur-de-Lis abdominoplasty. This is like a full abdominoplasty with the addition of a long vertical scar to improve the horizontal laxity that patients present with. As in Wise pattern in breast, you must address both horizontal and vertical laxity. The key is to achieve superior results in exchange to scars

Reverse Abdominoplasty
This technique is indicated for patients complaining of skin redundancy in the upper abdomen. It is also used in patients that have undergone traditional abdominoplasty in the past and have unsatisfactory results. It is very commonly used in conjunction with breast surgery as the scars are placed in the inframammary fold.
No-Drain Abdominoplasty with Progressive Tension Sutures
This technique eliminates the need for postoperative drains. The approach is the same as described above with the difference that sutures are used to “coapt” the tissue surfaces and close the “dead’ space.
Revision Abdominoplasty
Body contouring has advanced significantly and as such, more procedures are performed over the most recent years increasing also the procedures that need revision. The most common reasons for revision are:
Complications
Seromas are one of the most common complications and are treated with serial aspirations.
Bleeding can vary from a small hematoma to extensive bleeding. Take back to surgery and surgical drainage of hematomas is most of the times the treatment of choice
Delayed wound healing is not uncommon and is treated locally with dressing changes as needed and is self-limiting.
Surgical technique is one of the most important factors to achieve aesthetically pleasing scars. But in some cases, scarring will still occur. The decision to proceed with scar revision is usually taken 1 year after surgery
Postoperative anticoagulation and early ambulation are used to avoid thrombotic events. The dose and duration of the anticoagulation is based on patient traits and surgeon preference